
- Summary
- If a protocol is just a document, why does writing it take so long?
- Where does the synopsis-to-protocol journey encounter the most friction?
- How does the medical writer’s role extend beyond writing?
- Can AI really help medical writers, or is this just hype?
- How does Clinion eProtocol illustrate an AI‑assisted workflow?
- Are organisations actually using AI for protocols yet?
- What worries teams about AI‑assisted authoring?
- How can teams adopt AI responsibly without jeopardising quality?
- What’s the most important takeaway for protocol teams considering AI?
- Take a Closer Look
Summary
Clinical protocol writing is often described as a paperwork exercise. In reality, the most demanding part is aligning decisions across disciplines: science, operations, statistics, safety and regulation.
This Q&A draws on Clinion’s webinar From Synopsis to Protocol: Re‑examining the Medical Writer’s Workflow in the Age of AI and the accompanying e‑book, but it goes further by weaving in real‑world examples and poll insights. The goal is to show what truly slows down protocol development, where artificial intelligence (AI) can help, and why human expertise remains irreplaceable.
If a protocol is just a document, why does writing it take so long?
It isn’t just a document. A protocol is the blueprint for how a trial will run. It must capture the scientific objectives, define who is eligible, specify how data will be collected and analysed, anticipate risks, and satisfy regulatory requirements. Those decisions are rarely finalised when a synopsis is first drafted. A synopsis might say “collect safety labs regularly,” but not specify which labs, when, for which subgroups, or how those samples interact with visit windows. Writers must chase those details down, interpret them, and weave them into one coherent story.
In the webinar, 51% of respondents said the biggest drain on time is resolving ambiguity and aligning stakeholders [Fig. 1].
That statistic reflects everyday reality: the hardest part is not typing prose but reconciling differences. For example, the clinical team might think of progression‑free survival (PFS) as the primary endpoint in an oncology study, while biostatistics assumes overall survival (OS). Clarifying which endpoint drives the analysis can take days of discussion and revises multiple sections. The writer’s role is to surface such misalignments before they derail the draft.

Fig: 1
Where does the synopsis-to-protocol journey encounter the most friction?
Teams often assume drafting is the biffest hurdle, but the real slowdowns occur upstream and downstream of writing:

Fig. 2
Ambiguity in the starting point:
Synopses are concept documents. They often omit secondary endpoints, eligibility nuances, or sample size assumptions. Even seemingly small ambiguities, such as how a study population is defined, can trigger extensive clarification and affect ethics submissions, recruitment strategies, and operational planning.
Conflicting inputs from stakeholders:
Clinical, safety, regulatory, and statistical groups each bring their own priorities. A trial might propose broad eligibility to maximise enrolment, while the safety team insists on tighter criteria. Achieving consensus requires diplomacy and often multiple meetings. In one project, operations wanted daily remote monitoring visits, while sites insisted weekly was more practical. Resolving that clash delayed the draft by three weeks.
Hunting for information:
Key data lives in investigator brochures, historical protocols, sponsor templates and email threads. Writers spend hours checking whether the latest safety language is version 3 or version 4, or whether the template has changed since the last study.
This manual search is why 20% of poll respondents [Fig. 1] cited scattered information as a major pain point.
Synchronising revisions:
When one section changes, others must follow. A change in randomisation ratio alters the sample size rationale, schedule of assessments, and statistical analysis plan. Without an impact‑analysis tool, these knock‑on effects are easy to miss. Inspection teams often ask for evidence of who approved a change and when; tracking that history through emails can be difficult.
Ensuring traceability:
Regulators expect a clear link between the protocol and its sources. When a sponsor modifies an exclusion criterion based on new literature, inspectors want to see the reference and approval chain. Maintaining citations, document histories and review notes is administratively heavy.
These pain points illustrate why protocols are not simply written; they are negotiated and curated. A writer’s time is often consumed by decision integration and quality control rather than original prose.
How does the medical writer’s role extend beyond writing?
Medical writers are much more than scribes. They act as translators, integrators and custodians:
Translator:
They convert scientific intent into operational language. For example, turning “evaluate efficacy” into specific endpoints and visit schedules. They ensure clinical terminology is accessible to site staff and regulators.
Integrator:
Writers synthesise input from clinicians, statisticians, regulatory affairs, safety, operations and supply chain. They resolve conflicting definitions (e.g., what constitutes “disease progression”) and harmonise terminology.
Mediator:
Writers broker compromises when functions disagree. In practice, this means convening calls, drafting alternative wording, capturing decisions and documenting rationale. It is a diplomatic role as much as a writing one.
Custodian:
Writers safeguard consistency and compliance. They check that inclusion criteria match assessment schedules, that randomisation schemes align with sample size calculations, and that the document follows ICH GCP and sponsor templates. They also maintain version histories and citations for audit readiness.
In short, the writer owns the narrative integrity of the protocol. AI tools can speed up drafting and formatting, but they cannot judge whether an endpoint is appropriate or negotiate a compromise between conflicting stakeholders. Those tasks remain human‑centric.
Can AI really help medical writers, or is this just hype?
AI can assist with the workflow, not replace the expertise. Purpose‑built tools are emerging that focus on reducing manual effort around drafting, retrieval and consistency, while leaving decisions to people. The most useful capabilities include:
Document ingestion and retrieval:
AI can ingest the synopsis, previous protocols and reference documents, extract key parameters and make them easily searchable. This addresses the “hunting for information” bottleneck.
Structured draft generation:
From the synopsis and references, the system can generate a first draft using standard templates (e.g. ICH M11 or TransCelerate). Starting from a structured draft allows writers to spend more time on content quality rather than formatting.
In the poll, 32% of attendees selected AI-assisted first-draft generation as the capability they valued most [Fig. 3].
Consistency checks and impact analysis:
When one section changes, AI can highlight related sections that may need updates. Automated reviewers can flag missing content, misalignments, or deviations from sponsor standards. This helps maintain integrity across iterations.
Prompt‑driven edits and reference support:
Writers can ask the system to “shorten the eligibility criteria” or “add a citation supporting the use of surrogate endpoints,” and AI will propose revisions or retrieve relevant literature. This reduces manual search and rephrasing.
Citation management and export:
AI can help maintain hyperlinked references, track version history and produce audit‑ready exports. Reviewers can see where each section came from and who approved it.

Fig. 3
These features are not meant to produce a protocol at the push of a button. They relieve writers of repetitive tasks, leaving more time for scientific judgement, stakeholder engagement, and risk assessment.
Simplifying Clinical Trial Protocol Development with GenAI
Explore how generative AI can help clinical teams streamline protocol development, reduce manual effort, and improve consistency across the authoring workflow.
How does Clinion eProtocol illustrate an AI‑assisted workflow?
Clinion eProtocol is one example of a platform designed around the friction points above. It uses multiple AI agents to support, not replace, medical writers. Each agent is focused on a specific step:
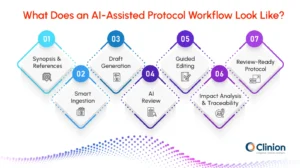
Fig. 4
Smart ingestion:
Upload the synopsis and references; eProtocol extracts key study details into a secure project workspace. This speeds up information retrieval.
Draft generation:
The authoring agent produces a structured protocol draft aligned with ICH M11/TransCelerate and sponsor templates. It proposes applicable sections, populates standard content and uses consistent terminology.
AI review:
A reviewing agent checks the draft against regulatory expectations and internal SOPs, flagging missing sections or misaligned language. It does not approve content; writers still review and resolve flagged items.
Edit assistant:
Writers can refine sections through prompt‑based commands, and all changes are tracked with user attribution. This encourages targeted revisions rather than repeated reformatting.
Impact analysis and traceability:
When a change is made, the system highlights downstream effects and updates citations. A full audit trail records who made which change and why.
This agentic design allows AI to handle tedious tasks while keeping humans in control of decisions. It is not the only approach, but it illustrates how AI can be integrated responsibly into an authoring workflow.
Are organisations actually using AI for protocols yet?
Adoption is cautious but growing. In the webinar poll, 46% of respondents said they are not yet exploring AI for protocol or medical writing, and 44% are still evaluating it [Fig. 5]. Only a small minority reported piloting AI in select studies.
This mirrors conversations across the industry: teams are intrigued by the promise of efficiency but wary of compliance risks. Many start by testing AI on low‑risk documents (e.g. lab manuals or early drafts) before applying it to core protocols.
The primary driver is not speed alone. Teams want to reduce rework and increase traceability. AI‑assisted impact analysis and first‑draft generation were ranked as key benefits by the audience, but adoption will only accelerate if vendors can demonstrate robust data privacy, validation and integration with existing systems.
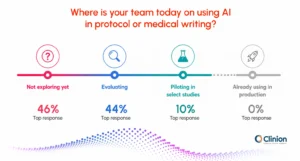
Fig. 5
What worries teams about AI‑assisted authoring?
Data protection tops the list. Protocols contain sensitive information about investigational products and proprietary study designs.
In the poll, 50% ranked data privacy and isolation as their main adoption consideration [Fig. 6].
Organisations want assurances that their documents will remain segregated, encrypted and not used to train public models.
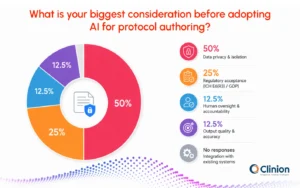
Fig:6
Beyond privacy, teams worry about:
Regulatory acceptance:
Will regulators trust a protocol generated with AI assistance? Sponsors must be prepared to document how AI was used and show that humans reviewed and approved the final content.
Human control:
Teams must avoid the temptation to accept AI output uncritically. Writers and reviewers need clear workflows to accept, reject, or modify suggestions.
Output quality:
AI can occasionally hallucinate or miss nuance. If a hallucinated reference or outdated guideline is inserted, it could undermine the protocol. Robust validation and testing are essential.
Systems integration:
AI tools need to work with existing document management systems, templates and approval workflows. A standalone AI authoring tool that creates parallel processes will struggle to gain traction.
These concerns highlight the need for strong governance, clear policies and technical safeguards as teams experiment with AI.
Unlocking Faster Study Start with eProtocol Automation
Learn how eProtocol automation can help clinical teams accelerate study start-up, reduce manual protocol workflows, and improve consistency from planning to execution.
How can teams adopt AI responsibly without jeopardising quality?
Responsible adoption starts with the premise that AI outputs are drafts, not final documents. Human oversight should be non‑negotiable. Other principles include:
Clear governance:
Define which documents and tasks AI can support, who reviews AI suggestions and how approvals are documented. Start with pilot projects, then expand as confidence grows.
Data hygiene:
Understand what data enters the AI pipeline, how it is stored, and who has access. Use project‑level data isolation, encryption and role‑based access control.
Transparency and traceability:
Systems should record prompts, sources and version histories. Writers and auditors must be able to see how a section was generated or revised.
Benchmarking against regulatory templates:
Evaluate AI output against standards such as ICH GCP and ICH M11. Automated reviewers can help, but final sign‑off must come from qualified experts.
Iterative rollout:
Begin by using AI for narrow tasks like generating background sections or managing citations. As trust grows, expand to more complex sections. Avoid “big bang” adoption.
By following these guidelines, teams can experiment with AI without sacrificing scientific rigour or regulatory compliance.
What’s the most important takeaway for protocol teams considering AI?
The core insight from the webinar and e‑book is that protocol writing isn’t really about writing; it’s about decision integration. AI can help by automating the tedious parts of document assembly, retrieving information quickly, checking for consistency and suggesting edits. But AI does not make the final decision on whether an endpoint is clinically meaningful, reconcile divergent opinions, or assume regulatory accountability. Those responsibilities remain with the medical writer and study team.
Take a Closer Look
If you’d like to dive deeper into the topic, the full ebook From Synopsis to Protocol: Re‑examining the Medical Writer’s Workflow in the Age of AI provides a detailed breakdown of the process, more poll results, sample workflow diagrams and a comparison of traditional versus AI‑assisted authoring.
Disclosure: This article is informed by content from Clinion’s webinar and eBook but is not a verbatim summary. It is a synthesis of key questions and answers intended to help teams understand the evolving landscape of protocol authoring and AI.
Want to see AI-assisted protocol authoring in action?
Watch the webinar recording to explore key Q&A insights on AI and medical writing, or request a demo to see how Clinion eProtocol helps teams move from synopsis to review-ready protocol faster.


