
- Summary
- Overview
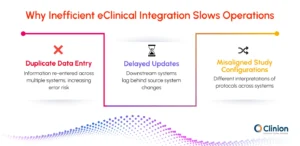
- Why Disconnected eClinical Systems Create Operational Delays
- What an Integrated eClinical Platform Actually Means
- Understanding Workflow Interactions in Modern Clinical Trial Execution
- Why Protocol Amendments Expose Workflow Gaps
- Operational Impact of Integrated eClinical Systems
- What to Evaluate in an Integrated eClinical Platform
- The Reality of Implementing Integrated eClinical Platforms
- Conclusion
- External References
Summary
Integrated clinical platforms unify disconnected eClinical systems into seamless workflows. They maintain real-time synchronization throughout the trial lifecycle, reducing startup time, accelerating amendments, eliminating duplicate entry, and improving operational visibility across all trial functions.
Overview
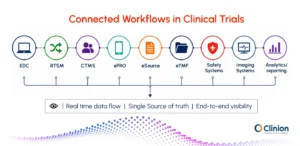
Clinical trials today rarely operate within a single system. Study teams work across Electronic Data Capture (EDC), Randomization and Trial Supply Management (RTSM), ePRO platforms, CTMS environments, safety systems, analytics tools, and document repositories throughout the trial lifecycle. While these technologies support different operational functions, the workflows between them often remain disconnected.
A protocol amendment, for example, may require updates across visit schedules, randomization workflows, patient-facing systems, supply planning, and downstream reporting structures. In many organizations, these changes still rely on manual coordination between teams and systems. The result is not always a lack of technology, but it is the operational friction that is created between technologies.
This challenge is showing a growing interest in integrated eClinical platforms that support connected clinical trial workflows.
Why Disconnected eClinical Systems Create Operational Delays
Even though clinical trial environments have become increasingly digital in the past decade, the operational teams still spend significant time on data reconciliation and managing workflow dependencies across separate systems. The issue is especially visible in large global studies where there are multiple functional teams working simultaneously.
Systems Often Operate Independently
Clinical trials rely on multiple e-clinical platforms throughout the study lifecycle, and each supports a different operational function.
Workflow Area | System Used | What It Typically Handles |
Clinical data collection | EDC | Site-entered patient data, edit checks, queries |
Trial management | CTMS | Site tracking, milestones, monitoring activities, and finance |
Patient participation | ePRO/eCOA | Patient questionnaires, symptom reporting, and diaries |
Randomization & drug allocation | RTSM/IWRS | Treatment assignment and supply coordination |
Safety management | Pharmacovigilance systems | Adverse event review and regulatory reporting |
Trial documentation | eTMF | Essential study documents and audit records |
In connected clinical trial workflows, information moves continuously between these systems as study activities progress. For example, when a patient is enrolled in EDC, that information may also need to flow into:
- randomization workflows in RTSM,
- monitoring activities in CTMS,
- patient schedules in ePRO systems,
- and downstream supply planning.
If those updates do not synchronize efficiently, study teams often step in manually to reconcile data, validate statuses, or coordinate operational changes across systems.
Workflow Friction Occurs Between eClinical Systems
Disconnected clinical trial systems commonly create operational pressure in areas such as:
- duplicate data entry,
- delayed downstream updates,
- inconsistent study configurations,
- repetitive reconciliation activities,
- fragmented operational visibility.
For example, if enrollment information in EDC does not synchronize efficiently with RTSM workflows, operational teams may spend additional time validating subject statuses and treatment assignments. Similarly, when ePRO data remains isolated from broader clinical datasets, review teams lose continuous visibility into patient-reported outcomes.
These issues become more visible during mid-study changes, accelerated timelines, or large multi-site trials where workflow coordination becomes increasingly dependent on system connectivity.
Workflow Gaps Affect Clinical Trial Execution
Workflow fragmentation affects not just individual operational tasks, but also trial activities as they move from one stage to another.
Disconnected workflows can slow:
- study startup,
- amendment implementation,
- centralized monitoring,
- safety review,
- database lock preparation,
- downstream reporting readiness.
The impact is particularly noticeable when teams rely on email-based coordination or spreadsheet tracking to bridge operational gaps between systems.
What an Integrated eClinical Platform Actually Means
Integrated eClinical platforms are often described as unified technology ecosystems, but the value of integration extends beyond system connectivity. The goal is to maintain workflow continuity across the trial lifecycle.
Integration Is More Than Data Exchange
Some organizations operate with multiple systems connected through APIs or periodic data transfers. While this may support basic interoperability, it does not necessarily create operational continuity.
True workflow integration allows:
- downstream systems to remain aligned,
- operational activities to update cohesively,
- teams to work from synchronized study information.
This distinction matters because disconnected workflows often create delays during protocol amendments, enrollment changes, safety escalations, or reporting preparation. Integrated eClinical platforms aim to reduce those operational gaps through continuous coordination between systems and trial functions.
Understanding Workflow Interactions in Modern Clinical Trial Execution
The effectiveness of an integrated eClinical platform depends on how well different systems support connected trial activities. Clinical workflows often move between platforms such as EDC, RTSM, ePRO, CTMS, and safety systems throughout study execution. Understanding how these systems interact helps explain why integration plays an important role in trial coordination, data continuity, and operational efficiency.
Protocol Authoring and EDC Setup
Protocol design is one of the earliest dependencies in clinical trial execution because it influences how multiple downstream systems are configured during study startup. Information defined in the protocol, such as:
- visit schedules,
- schedule of assessments,
- eligibility criteria,
- endpoint definitions,
- study procedures,
must eventually be reflected in EDC structures, patient visit schedules, data collection workflows, and operational tracking activities.
When protocol authoring and EDC setup operate independently, study teams often recreate these structures manually across systems. This not only increases setup effort but also introduces interpretation gaps between the approved protocol and the operational study environment.
Even small inconsistencies in visit windows, assessment schedules, or form structures can create downstream issues. Well-integrated workflows help maintain alignment between protocol requirements and study configuration activities, which reduces repetitive setup work and improves consistency across downstream trial systems.
EDC and RTSM
Enrollment and randomization workflows are closely connected during study execution. Once a subject is enrolled in EDC, that information often needs to trigger treatment assignment and supply-related activities within RTSM. This interaction supports:
- subject randomization,
- treatment allocation,
- cohort assignment,
- investigational product tracking.
When EDC and RTSM workflows are not aligned properly, study teams may need to manually re-enter subject information, reconcile enrollment statuses, or validate treatment assignments across systems. These inefficiencies can increase operational burden during enrollment while also creating inconsistencies between clinical and supply workflows.
The impact becomes more visible in blinded studies, adaptive trials, or high-enrollment programs where delays in synchronization can affect both operational oversight and supply continuity.
Learn how Clinion’s unified EDC-RTSM workflows help reduce manual coordination during study execution.
Drug Supply Coordination Through RTSM
Drug supply planning depends heavily on accurate and continuous coordination between randomization activity and inventory management workflows. As subjects are enrolled and treatment assignments are generated, supply systems must account for:
- site inventory levels,
- dispensing activity,
- resupply timelines,
- kit allocation requirements.
Disconnected workflows can create delays in inventory visibility or increase the likelihood of supply imbalances across sites. In global studies where investigational product movement must remain aligned with changing enrollment patterns across regions, these challenges become particularly important.
Explore how Clinion RTSM helps support connected randomization and drug supply workflows across global clinical trials.
Learn more about Clinion RTSM →
ePRO/eCOA and EDC
Patient-reported outcomes are becoming important in clinical trials, particularly in decentralized and hybrid study models where patient participation extends beyond site visits.
Data collected through ePRO/eCOA platforms often needs to remain aligned with:
- scheduled study visits,
- subject timelines,
- endpoint assessments,
- broader clinical review workflows.
This integration is important because patient-reported data contributes directly to clinical endpoints and supports a more complete understanding of patient experience alongside site-collected data in EDC.
In decentralized and hybrid trials, ePRO/eCOA data may also contribute to real-world evidence (RWD) generation by capturing patient experiences in more naturalistic, real-time settings outside traditional site visits. This increases the importance of aligning patient-reported data with core clinical datasets during review and analysis.
When ePRO/eCOA systems operate separately from EDC, study teams may face delays in identifying missing assessments, tracking patient compliance, reconciling visit-related data, and reviewing patient-reported outcomes alongside clinical observations. Well-integrated workflows help maintain continuity between patient-generated data and broader clinical datasets, improving visibility across study activities.
Explore how ePRO integration with EDC supports connected patient workflows.
Read more →
eSource and EDC
Site staff often work with both source documentation and EDC entry during clinical trial execution, especially in sites handling high patient volumes or complex protocols.
When eSource and EDC operate as separate workflows, site coordinators typically need to manually transcribe information from source records into EDC systems. This increases administrative workload and introduces a higher risk of transcription discrepancies between source documents and the clinical database.
These challenges become more significant in studies involving:
- high patient enrollment rates,
- frequent or repeated assessments per visit,
- complex visit structures with multiple data points.
In addition, manual entry can create delays in data availability for downstream review, as data must be re-entered, verified, and queried before it becomes analysis-ready. An integrated system helps reduce duplicate data entry by enabling structured source data capture that can flow directly into the clinical database.
EDC and Medical Coding/Safety Systems
Safety workflows depend on continuous and accurate movement of adverse event and medication data between clinical and pharmacovigilance systems. Information captured in EDC typically feeds into:
- adverse event review and assessment,
- medical coding and dictionary mapping (e.g., MedDRA, WHO Drug),
- safety case processing and validation,
- regulatory reporting and submission workflows.
When EDC and safety systems operate independently, safety teams often need to manually extract, reformat, or reconcile clinical data before it can be processed in pharmacovigilance systems. This creates additional handling steps between data capture and regulatory reporting. These manual dependencies can slow safety review timelines and increase operational effort during ongoing case processing, particularly in studies with frequent adverse event reporting.
More connected workflows help enable faster and more consistent transfer of safety-related data from EDC to pharmacovigilance systems. This improves alignment between clinical data and safety databases while supporting more efficient case processing and reporting workflows.
CTMS and EDC
Clinical operations teams rely on both CTMS and EDC to monitor study progress and ensure execution aligns with planned milestones. These systems support closely linked oversight activities, including:
- subject enrollment tracking,
- site activation and performance monitoring,
- visit and milestone completion tracking,
- monitoring visit planning and follow-up,
- overall study progress visibility.
When CTMS and EDC operate in isolation, teams often depend on manual updates or periodic data refresh cycles to align operational and clinical information. This creates gaps in real-time visibility across study execution. These gaps can make cross-functional coordination more difficult, particularly in large multi-site or global studies where operational decisions depend on timely and accurate study status information.
EDC and Analytics / Reporting
Clinical reporting and analytics workflows depend on consistent, structured, and continuously updated, high-quality data from EDC systems
Information captured in EDC typically contributes to:
- operational dashboards and trial metrics,
- centralized data review and cleaning workflows,
- query tracking and resolution monitoring,
- interim and final study reporting preparation.
When analytics platforms rely on manual extraction or periodic data transfers from EDC, reporting workflows become more time-consuming and require repeated reconciliation of datasets across systems. This can also delay access to study insights required for operational monitoring, data review meetings, and executive-level decision-making.
More integrated data environments help ensure that EDC data flows directly into analytics systems with minimal manual handling. This improves data consistency, reduces reporting lag, and supports more efficient preparation of downstream analyses and submission-ready datasets.
eConsent and EDC
Consent workflows play an important role in subject enrollment and study participation during clinical trials. Information collected through eConsent platforms often needs to remain aligned with:
- subject records,
- screening activities,
- eligibility confirmation,
- visit workflows managed within EDC systems.
When eConsent and EDC workflows operate separately, study teams may need to manually verify consent status, document versions, or enrollment readiness across systems before subjects can proceed further in the study. This creates additional coordination effort during screening and onboarding activities.
The impact becomes more visible in decentralized and multi-site trials where consent workflows may occur remotely across different patient environments and timelines.
More connected eConsent and EDC workflows help maintain better continuity between patient consent activities and downstream clinical operations while improving visibility into subject readiness during enrollment.
EDC and CSR Automation
In modern clinical trials, the EDC system serves as the primary source of patient-level clinical data used across downstream reporting and analysis workflows. Data captured in EDC often contributes to:
- analysis datasets such as CDISC SDTM and ADaM,
- tables, listings, and figures (TLFs),
- patient summaries,
- downstream Clinical Study Report (CSR) preparation.
When analytics and reporting environments remain disconnected from EDC, study teams often spend significant time manually extracting, reconciling, validating, and reformatting data before reporting activities can move forward. These dependencies can increase operational effort during study closeout and slow reporting timelines, particularly in studies involving large datasets or multiple protocol amendments.
More connected workflows help maintain stronger continuity between EDC data and downstream reporting systems, improving readiness for analysis and reducing reconciliation effort during CSR preparation.
However, CSR development still depends on medical writing, clinical interpretation, and cross-functional review activities. Automation primarily supports structured data preparation and reporting workflows rather than generating a complete CSR independently.
eTMF, CTMS, and EDC Workflows
Clinical trial documentation depends on continuous coordination between operational, clinical, and regulatory activities throughout study execution. CTMS and EDC workflows often generate:
- study milestones,
- monitoring activities,
- enrollment updates,
- site-level operational records,
- trial execution data linked to documentation workflows.
This information frequently contributes to documentation maintained within eTMF systems throughout the study lifecycle.
When these systems operate independently, study teams may need to manually track document status, reconcile operational activities, or coordinate updates across multiple environments. This can reduce visibility into documentation readiness during monitoring, audit preparation, or study closeout.
The challenge becomes more significant in large global studies where documentation workflows continue evolving alongside ongoing operational activity across sites and regions.
More connected workflows help maintain better alignment between study execution and trial documentation while improving continuity across operational and regulatory processes.
EDC and Imaging Systems
Many clinical trials rely on imaging data as part of endpoint evaluation, centralized review, or safety assessment workflows. Imaging repositories often operate alongside EDC systems to manage:
- radiology assessments,
- cardiology imaging data,
- endpoint-related image review workflows,
- image-based safety evaluations.
When imaging workflows remain disconnected from broader clinical datasets, study teams may need to manually coordinate subject identifiers, visit timelines, review status updates, or imaging assessments across systems. This can increase operational effort during data review and reduce visibility into imaging-related workflow progress.
These challenges become more visible in studies where imaging endpoints influence treatment evaluation, eligibility assessment, or ongoing clinical review activities.
More connected workflows help maintain better continuity between imaging systems and clinical datasets while supporting more efficient coordination across review and operational teams.
See how integrated imaging and EDC workflows improve visibility across image review and clinical data.
Explore fully integrated medical imaging within your EDC system.
Why Protocol Amendments Expose Workflow Gaps
Protocol amendments often reveal weaknesses in disconnected eClinical systems more clearly than routine trial activities because they force multiple systems to change at the same time in a very short window.
A single amendment may affect:
- EDC structures,
- visit schedules,
- RTSM workflows,
- patient-facing systems,
- supply planning,
- reporting configurations.
When systems are not integrated, each of these updates is handled separately by different teams. This creates a dependency on manual coordination to ensure that every system reflects the same version of the protocol. The complexity is not just in making the changes, but in ensuring that no system is missed or updated incorrectly.
This is where workflow gaps become visible. Even small delays or mismatches in implementation can lead to inconsistencies between systems, which then affect downstream activities. Connected workflows reduce this risk by ensuring that protocol changes propagate more consistently across systems, keeping operational execution aligned with the updated study design.
Operational Impact of Integrated eClinical Systems
The value of integrated eClinical platforms becomes more visible when evaluating operational outcomes across the trial lifecycle.
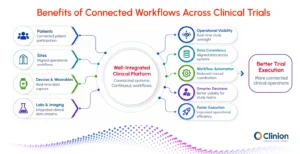
Study Startup:
Faster study builds through aligned configuration across EDC, CTMS, RTSM, and other systems, reducing setup inconsistencies and rework
Reconciliation & Coordination:
Reduced duplicate updates, fewer manual validations, and lower cross-system coordination effort across teams
Cross-Functional Visibility:
More continuous access to synchronized study data, improving coordination between clinical operations, data management, and medical review teams
Site Burden:
Reduced duplicate data entry and transcription effort, improving operational efficiency at site level
Review & Reporting Readiness:
Cleaner and more consistent data flow into reporting systems, reducing late-stage aggregation effort and improving readiness for interim and final analysis.
What to Evaluate in an Integrated eClinical Platform
As organizations evaluate integrated eClinical platforms, the focus shifts from individual system features to how effectively those systems work together across clinical trial execution.
Workflow-Level Integration
Evaluation should focus on whether systems support end-to-end trial workflows rather than functioning as loosely connected tools. The key is not just data transfer between systems, but how smoothly operational activities move across EDC, CTMS, RTSM, ePRO, and other platforms during study execution.
Unified User Experience
A fragmented user experience often results in frequent switching between systems for both site users and study teams. A unified interface reduces this operational switching and helps maintain continuity in daily trial activities, particularly in high-volume or multi-study environments.
Configurability and Scalability
An effective platform should support different study designs without requiring structural changes to core workflows. This becomes critical for global studies, adaptive designs, decentralized components, and long-duration programs. Scalability is equally important when organizations need consistency across multiple concurrent studies.
Real-Time Operational Visibility
Operational oversight depends on having timely and aligned information across all trial systems. This includes visibility into enrollment progress, site performance, monitoring activity, and safety-related updates. Delayed or fragmented data visibility can directly affect decision-making during study execution.
Compliance and Traceability
Integrated systems must maintain regulatory compliance across all connected workflows. This includes audit trails, controlled user access, electronic record compliance, and consistent data governance across systems. As integration depth increases, maintaining traceability across data flows becomes more important.
Readiness for Automation and AI
Automation and AI-driven capabilities depend on the availability of consistent, connected datasets across clinical systems. Strong integration enables use cases such as automated reporting, coding support, and predictive analytics, where performance is directly influenced by data continuity and accessibility.
The Reality of Implementing Integrated eClinical Platforms
While integrated eClinical platforms improve operational continuity, implementing them across clinical environments involves multiple layers of complexity. Most organizations operate within established systems and long-standing study processes, which makes aligning workflows across platforms a gradual and structured effort.
Integration is not only about connecting systems technically. It also depends on how data is structured, how processes are designed across functions, and how consistently those workflows are adopted across studies. Differences in setup approaches and operational practices can create variation in how smoothly integration works in real-world execution.
Beyond system alignment, adoption plays a major role. Moving from independent tools to connected workflows requires changes in how teams interact with data and with each other. This shift often takes time, especially in environments where multiple studies run in parallel with different operational models.
Conclusion
As integrated eClinical platforms become more widely adopted, evaluation is shifting from individual system capabilities to how well systems support end-to-end trial execution. The focus is on workflow continuity rather than module coverage alone.
For organizations ready to move beyond disconnected systems, the question is no longer whether to integrate, but how to prioritize integration investments to deliver the highest operational value. Those starting this journey should focus first on the workflows where friction is most visible, such as study startup and protocol amendments, then expand integration systematically across other trial functions.
Clinion: Unifying Clinical Trial Operations Through AI-Powered Integration
Clinion’s AI-enabled eClinical platform brings together a unified suite of clinical trial solutions, including EDC, RTSM, CTMS, eConsent, ePRO, eSource, eProtocol Automation, CSR Automation, and eTMF. By connecting these functions within a single ecosystem, the platform helps reduce operational fragmentation and supports smoother continuity across different stages of clinical trial execution, from study setup through reporting.
External References
The Integration of Clinical Trials with the Practice of Medicine: Repairing a House Divided - PMC
The Benefits of Integrating Clinical Trials at the Community Level
Raising the Standards for Clinical Integration | Applied Clinical Trials Online
Integrating Clinical Research and Practice: Examples
Integrating eConsent With EDC Streamlined Workflows For Seamless Trials
Integrating EHR with EDC: When Two Worlds Collide | Applied Clinical Trials Online


